– Dr Hemant Baonerkar


Introduction
A cyst can be defined as a benign pathologic cavity within bone or in soft tissues, generally formed by a connective tissue wall. The cavity, within the oral regions, is almost always lined by dental epithelium. Some cyst-like lesions, without epithelial lining, also can be seen in the maxillo-facial regions. The cyst's lumen usually contains fluids, keratin or cellular debris (pus) or gas. Treatment of cysts varies from curettage, excision, enucleation, marsupalization depending on nature and size of the cyst.

Dentigerous cyst is a developmental odontogenic cyst. It is the second most common cyst in jaws, accounting for 20% of all jaw cysts cases. Generally it is more common in males than females, and most common site is body of mandible and posterior mandible. It usually presents between 10 and 30 years of age and is mostly associated with deep seated impacted wisdom tooth. Dentigerous cysts are usually non aggressive and asymptomatic, unless infected. The objective of this article is to present a case of a dentigerous cyst with its clinical, radiological features, and its treatment plan.
Case Report
A 55 year old female patient reported to the hospital with chief complaint of pain and swelling in mandibular left posterior region from last 6 months. Patient reported that initially the swelling was asymptomatic but gradually increased in size, causing pain and discomfort. She did not have any relevant medical history.
On intraoral examination, swelling in mandibular wisdom tooth region and anterior ramus was present. Buccal cortical expansion from mandibular left second molar to ramus area was found. Small intraoral draining sinus was also present. Same area had moderate inflammation. Extraoral tenderness on palpation was present at left angle of mandible and ramous region. Patient was advised to do radiographic evaluation.
Radiographic evaluation
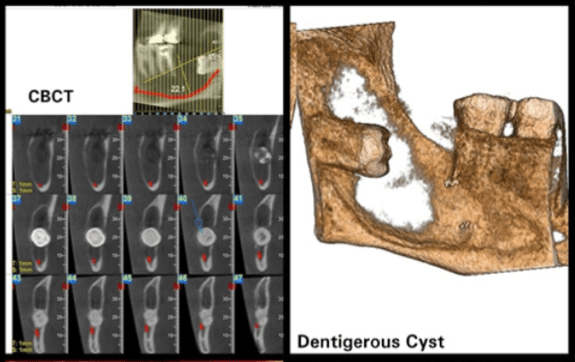
CBCT (cone beam computerized tomography) scans showed a well defined radiolucency present with impacted mandibular left wisdom tooth, extending from the periapical region of second molar to distal to third molar. A well defined radiolucency surrounded by radio opaque boundaries is the classical radiological presentation of cystic pathology.
Osteolytic activity was diagnosed on both, the buccal and lingual cortex. Thinning of buccal bone cortex and resorption with perforation on lingual cortex was suggestive of chronic cystic pathology. Crown of wisdom tooth encircled in radiolucency was suggestive of dentigerous cyst. Size of pathology anterio posteriorly was approximately 29 mm and superio inferior was approximately 22.1 mm. Moderate buccal cortical expansion was present. Due to pathologic expansion, inferior alveolar nerve was pushed downward and wisdom tooth was pushed distally in ramus, suggesting pathology is benign but locally aggressive. (Image no. 1)

Differential diagnosis
Based on the above findings differential diagnosis for this case was
- benign odontogenic cyst
- dentigerous cyst
- unicystic ameloblastoma
- keratocyst etc.
Lab investigations
Lab investigations such as
- complete blood count (CBC)
- blood sugar levels and
- viral markers
were done and they were in normal reference limits.
Surgical procedure
Surgical procedure was planned under general anesthesia. Local infiltration of lignocaine and adrenalin was administered at surgical site to achieve hemostasis and local effect. An intraoral incision was places with no. 15 surgical blade. Intraoral full thickness mucoperiosteal flap was raised from first molar up to distal and buccal to ramus region. Then, enucleation of cyst was done with Lucas curette. (Image no.2)

The extraction of impacted wisdom tooth was completed. Complete cystic lining was removed. (Image no 3)

Peripheral osteotomy was done with a round HP 08 bur (Image no. 4) to prevent recurrence.

Debridement of the pathologic defect was done with 10% betadine solution. (Image no 5)

Closure was achieved with 3-0 vicryl suture material. After reversal of GA by anesthetist, patient was shifted to the recovery room.
Post operative medication, like antibiotics and analgesics was given via IV line.
Histopathological examination
The pathological specimen was sent to the pathology lab. Histopathology confirmed the presence of a thin, non-keratinized stratified squamous cuboidal epithelial lining, with inflammatory cells and mucus cells, suggestive of dentigerous cyst. (Image no 6)

Discussion
A cyst is a closed, sac-like structure that contains fluid, gas, or semisolid material and is not a normal part of the tissue where it is located. Cysts are common and can occur anywhere in the body in people of any age. Cysts vary in size; they may be detectable only under a microscope or they can grow so large that they displace normal organs and tissues. The outer wall of a cyst is called the capsule.
A peri-apical (radicular) cyst is the most common tooth-derived cyst. A dentigerous cyst is a sac-like structure (in this case) derived from tooth-related tissues. It can be gas-filled, gel-filled or blood-filled but normally it is not pus-filled (that is, it is not normally/initially infected).
Stages of cyst –
- Infection
- Initiation
- Proliferation and
- Expansion
are the main stages of cyst.
Signs & symptoms- If small, the cyst is often not noticed. When larger though, teeth can become mobile. Cysts can become infected and this can be when it is first noticed by either dentist or patient. Dentigerous cyst are mostly asymptomatic and there’s pain only on infection.
Etiology – Dentigerous cyst is a developmental cyst. It forms around the crown of an unerupted or developing tooth. The epithelial lining originates from the reduced enamel epithelium after the crown has formed and calcified. Most commonly, it forms around the crown of an unerupted or impacted third molar.
Treatment options: Enucleation of cyst is the ideal treatment for small dentigerous cyst with extraction of causative tooth. Large cyst can be primarily marsupalized then secondarily enucleated. A smooth curettage is also recommended after extraction in order to eliminate any possible cystic remnant.
The treatment for a dentigerous cyst depends upon the size of the cyst along with its location. Cysts that are very large and result in symptoms due to their size may be surgically removed. Sometimes the fluid contained within a cyst can be drained, or aspirated, by inserting a needle or catheter into the cyst cavity, resulting in collapse of the cyst.
Conclusion
Surgical removal of a cyst is always necessary. Radiologic imaging must be used for accurate diagnosis. If there is any suspicion that a cyst is cancerous, the cyst is generally removed by surgery or a biopsy is taken of the cyst wall (capsule) to rule out malignancy.
The true treatment choice with the early clinical diagnosis of these lesions and treatment planning may increase the rate of success. A long-term follow-up is important for the diagnosis of the recurrence as well.
References
- Kirtaniya BC, Sachdev V, Singla A, Sharma AK. Marsupialization: A conservative approach for treating dentigerous cyst in children in the mixed dentition. J Indian Soc Pedod Prev Dent. 2010;28:203–8. [PubMed] [Google Scholar]
- Kalaskar RR, Tiku A, Damle SG. Dentigerous cysts of anterior maxilla in a young child: A case report. J Indian Soc Pedod Prev Dent. 2007;25:187–90. [PubMed] [Google Scholar]
- Tilakraj TN, Kiran NK, Mukunda KS, Rao S. Non syndromic unilateral dentigerous cyst in a 4-year-old child: A rare case report. Contemp Clin Dent. 2011;2:398–401. [PMC free article] [PubMed] [Google Scholar]
- Demirkol M, Ege B, Yanik S, Aras MH, Ay S. Clinicopathological study of jaw cysts in southeast region of Turkey. Eur J Dent. 2014;8:107–11. [PMC free article] [PubMed] [Google Scholar]
- Bharath KP, Revathy V, Poornima S, Subba Reddy VV. Dentigerous cyst in an uncommon site: A rare entity. J Indian Soc Pedod Prev Dent. 2011;29(6 Suppl 2):S99–103. [PubMed] [Google Scholar]
- Kozelj V, Sotosek B. Inflammatory dentigerous cysts of children treated by tooth extraction and decompression – Report of four cases. Br Dent J. 1999;187:587–90. [PubMed] [Google Scholar]















Comments