Abstract
One of the oldest and most prevalent disorders affecting people is dental caries. Newer approaches stress disease prevention and the preservation of tooth structure in light of the recent transition from the surgical model of disease management, which placed an emphasis on restorative therapy; to a medical model of disease management. Instead of waiting until a cavity forms and restorative therapy is required, this article discusses devices like DIAGNOdent, Digital Imaging Fiber-Optic Transillumination, quantitative light-induced fluorescence, and the Electronic Caries Monitor, used for early identification and monitoring of caries. Caries prevention strategies including oral hygiene practises, fluoridation, pit-and-fissure sealants, xylitol use, the development of a dental caries vaccine, and the role of the infant’s primary caregiver are also discussed. Key words: Dental caries, Risk assessment, Prevention, Diagnosis, and Detection


Introduction
Dental caries, a prevalent and persistent disorder, has historically been managed through surgical interventions involving decay removal and cavity filling. However, this approach often led to the progression of larger cavities and eventual tooth loss, particularly in lower socioeconomic groups. Recent advancements have shifted focus towards disease prevention and tooth structure preservation, transitioning from a surgical to a medical strategy. (1-3)

The development of dental caries is rooted in the transformation of oral biofilm microbiota due to frequent consumption of fermentable carbohydrates. This leads to the formation of an acidogenic, aciduric, and cariogenic biofilm population, causing erosion of dental hard tissues and the eventual formation of carious lesions. Dental caries is therefore viewed as a dietary-microbial disease, necessitating the presence of a cariogenic biofilm and regular exposure to fermentable carbohydrates. Fluoride plays a crucial role in prevention by aiding in remineralization and preventing demineralization, underscoring the importance of sufficient fluoride exposure in combating the disease. (4-7)
Early Childhood Caries (ECC) primarily affects primary teeth, particularly the maxillary anterior teeth, and is often triggered by prolonged exposure to sweetened beverages, especially before sleep or frequent consumption throughout the day.
ECC risk factors include pre-existing enamel hypoplasia and the vulnerability of newly erupted upper incisors, followed by molars and canines.
Rampant caries, characterized by extensive decay, affects multiple tooth surfaces and is associated with factors such as xerostomia, poor oral hygiene, stimulant usage, and high sugar consumption. Additionally, radiation-induced caries can occur after head and neck radiation therapy.
The development of caries at both individual and community levels is influenced by various factors, including bacterial colonization, family demographics, oral health practices, community dynamics, and access to dental care (8-14).
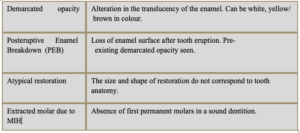
Molar-Incisor Hypomineralization (MIH) is marked by qualitative enamel defects, primarily affecting first permanent molars and associated incisors. Reduced activity of enamel-forming cells during enamel matrix formation and mineralization phases leads to the development of pits or grooves, presenting as hypoplasia or hypomineralization.
Diagnostic criteria for MIH, including demarcated opacities and enamel breakdown, were established by the European Academy of Paediatric Dentistry in 2003 (15-18).
Stages & Symptoms of Dental Caries
Progresses from initial mineral loss to irreversible cavity formation. (6)
l Stage of White Spots: Acid from bacteria destroys the mineral matrix of teeth, leading to the formation of chalky white patches on the tooth surface. At this stage, the lesion is reversible, and the surface remains intact. Distinguishing between early caries-induced white spots and developmental hypocalcification can be challenging.
l Cavity Stage: If mineral loss continues, the tooth surface eventually breaks or “cavitates,” resulting in irreversible damage. At this point, the lesion cannot be repaired, and large tooth areas may be lost. Active cavitated lesions typically appear golden brown, while long-lasting lesions may darken, sometimes appearing almost black. However, the color depth is not always indicative of lesion severity, as stopped decay can also be dark. (19)
Symptoms and signs of dental caries vary depending on the cavity size and location: (20)
- Toothache and dental sensitivity, especially after consuming sweet, hot, or cold foods or beverages.
- Visible cracks or holes in teeth.
- Brown, black, or white stains on tooth surfaces.
- Bad breath and unpleasant tastes.
Complications can include toothaches, pulpitis, tooth loss, and dental discoloration. In severe cases, life-threatening conditions such as cavernous sinus thrombosis and Ludwig angina may occur. (21)
Dental caries Detection and Prevention
Advancements in dental caries risk analysis and prediction have shifted focus from immediate cavity filling to managing plaque and promoting remineralization, thereby potentially reversing the caries process. (22) Traditional methods of caries diagnosis, such as radiography, tactile sensation, and visual inspection have limitations, particularly in detecting early enamel caries and assessing disease progression. However, recent technological innovations offer promising alternatives for early lesion detection and monitoring.(23)
- Laser fluorescence technology, exemplified by DIAGNOdent (24), enables the measurement of bacterial products in caries lesions with high sensitivity, aiding in the identification of early demineralization.
- Digital Imaging Fiber-Optic Transillumination (DIFOTI) (25) utilizes fiber-optic light to quantitatively characterize caries processes, potentially identifying early demineralization, fissures, or fractures.
- Similarly, Quantitative Light-Induced Fluorescence (QLF) (26)leverages enamel fluorescence under specific lighting conditions to detect demineralized areas
- The Electronic Caries Monitor (ECM) detects variations in electrical impedance between sound and demineralized enamel.
Assessing individual caries risk involves considering various factors such as calculus deposits, deep pits and fissures, snacking patterns, salivary flow, past caries experience, current caries index, and oral hygiene practices including fluoride use. These factors help predict the progression of dental caries and guide preventive strategies (23).
Preventive methods for dental caries encompass several approaches
- Maintaining good oral hygiene: Regular brushing, flossing, and rinsing help remove plaque, preventing periodontal disease and dental caries. Dentists can educate patients on proper oral hygiene techniques during routine checkups. (23)
- Fluoridation: Fluoride promotes remineralization of tooth enamel and inhibits demineralization, making teeth more resistant to acids and bacterial enzymes. Fluoride can be administered through water fluoridation, toothpaste, mouthwash, dietary supplements, and professional applications. (1)
- Pit and fissure sealants: Applied to molars and premolars, sealants fill deep pits and fissures, reducing plaque accumulation and susceptibility to caries. They are particularly beneficial for children and individuals with a high caries index. (27)
- Xylitol: Serving as a sugar alternative, xylitol can decrease the risk of cavities by reducing sucrose consumption, a known contributor to tooth decay. Incorporating xylitol into the diet can mitigate the harmful effects of sugar on dental health.(19)
- Vaccines: While commercial vaccines for dental caries prevention are not yet available, experimental vaccines targeting Streptococcus mutans aim to interfere with bacterial colonization and enzymatic activity. Clinical studies continue to investigate the feasibility and effectiveness of dental caries vaccines.(28,29)
- Role of primary caregivers: Parents, especially mothers, play a crucial role in preventing dental caries transmission to children. Practicing good oral hygiene and seeking dental care when necessary can reduce the microbial load of caries-causing bacteria, thus lowering the risk of caries in children. (13,14)
In summary, a comprehensive approach to dental caries prevention involves addressing individual risk factors, promoting good oral hygiene practices, utilizing fluoride, applying sealants, considering sugar alternatives, exploring vaccine development, and involving primary caregivers in maintaining oral health.
References
- Matthews P. Prevention of dental caries in children and young people. Nurs Child Young People. 2022 Nov 7. doi: 10.7748/ncyp.2022.e1451. Epub ahead of print. PMID: 36341704.
- Folayan, M.O., Adeniyi, A.A., Arowolo, O. et al. Risk indicators for dental caries, and gingivitis among 6–11-year-old children in Nigeria: a household-based survey. BMC Oral Health 22, 465 (2022). https://doi.org/10.1186/s12903-022-02470-1
- Schroë, S.C., Bonifacio, C.C., Bruers, J.J. et al. General and paediatric dentists’ knowledge, attitude and practises regarding the use of Silver Diammine Fluoride for the management of dental caries: a national survey in the Netherlands. BMC Oral Health 22, 458 (2022). https://doi.org/10.1186/s12903-022-02475-w
- Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, Tagami J, Twetman S, Tsakos G, Ismail A. Dental caries. Nat Rev Dis Primers. 2017 May 25;3:17030. doi: 10.1038/nrdp.2017.30. PMID: 28540937.
- Matthews P. Prevention of dental caries in children and young people. Nurs Child Young People. 2022 Nov 7. doi: 10.7748/ncyp.2022.e1451. Epub ahead of print. PMID: 36341704.
- Kidd EA, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83 Spec No C:C35-8. doi: 10.1177/154405910408301s07. PMID: 15286119.
- Pitts NB, Twetman S, Fisher J, Marsh PD. Understanding dental caries as a non-communicable disease. Br Dent J. 2021 Dec;231(12):749-753. doi: 10.1038/s41415-021-3775-4. Epub 2021 Dec 17. PMID: 34921271; PMCID: PMC8683371.
- Lam PPY, Chua H, Ekambaram M, Lo ECM, Yiu CKY. Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022 Oct 18;19(20):13459. doi: 10.3390/ijerph192013459. PMID: 36294037; PMCID: PMC9603429.
- Dr. Ramya JR, Dr. Rashi Singh, Dr. Nidhi Gupta, Dr. Natasha Gambhir, & 5. Dr. Divya Singh. (2022). Restoring The Candy Crushers – A Case Report On Ecc. A Journal of Advanced Dentistry Updent, 11(01), 19–22. https://doi.org/10.4880/zenodo.5930372
- Saikia A, Aarthi J, Muthu MS, Patil SS, Anthonappa RP, Walia T, Shahwan M, Mossey P and Dominguez M (2022) Sustainable development goals and ending ECC as a public health crisis. Front. Public Health 10:931243. doi: 10.3389/fpubh.2022.931243
- Tungare S, Paranjpe AG. Early Childhood Caries. 2022 Aug 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–. PMID: 30570970.
- Haresaku S, Kubota K, Miyoshi M, Obuse M, Aoki H, Nakashima F, Muramatsu M, Maeda H, Uchida S, Miyazono M, Iino H, Naito T. A Survey of Oral Assessment and Healthcare Education at Nursing Schools in Japan. Int Dent J. 2022 Nov 5:S0020-6539(22)00226-X. doi: 10.1016/j.identj.2022.09.006. Epub ahead of print. PMID: 36347715.
- Colak H, Dülgergil CT, Dalli M, Hamidi MM. Early childhood caries update: A review of causes, diagnoses, and treatments. J Nat Sci Biol Med. 2013 Jan;4(1):29-38. doi: 10.4103/0976-9668.107257. PMID: 23633832; PMCID: PMC3633299.
- Ripa LW. Nursing caries: a comprehensive review. Pediatr Dent. 1988 Dec;10(4):268-82. PMID: 3078603.
- Weerheijm KL. Molar incisor hypomineralisation (MIH). Eur J Paediatr Dent. 2003 Sep;4(3):114-20. PMID: 14529330.
- Mittal N, Sharma BB. Hypomineralised second primary molars: prevalence, defect characteristics and possible association with Molar Incisor Hypomineralisation in Indian children. Eur Arch Paediatr Dent. 2015 Dec;16(6):441-7. doi: 10.1007/s40368-015-0190-z. Epub 2015 Jun 20. PMID: 26092507.
- Garg N, Jain AK, Saha S, Singh J. Essentiality of early diagnosis of molar incisor hypomineralization in children and review of its clinical presentation, etiology and management. Int J Clin Pediatr Dent. 2012 Sep;5(3):190-6. doi: 10.5005/jp-journals-10005-1164. Epub 2012 Dec 5. PMID: 25206166; PMCID: PMC4155885.
- Abdalla, H.E., Abuaffan, A.H. & Kemoli, A.M. Molar incisor hypomineralization, prevalence, pattern and distribution in Sudanese children. BMC Oral Health 21, 9 (2021). https://doi.org/10.1186/s12903-020-01383-1.
- Sugars and dental caries [Internet]. [cited 2022 Nov 10]. Available from: https://www.who.int/news-room/fact-sheets/detail/sugars-and-dental-caries
- dental-caries-a-review.pdf [Internet]. [cited 2022 Nov 10]. Available from: https://www.alliedacademies.org/articles/dental-caries-a-review.pdf
- Mjör IA, Toffenetti F. Secondary caries: a literature review with case reports. Quintessence Int. 2000 Mar;31(3):165-79. PMID: 11203922.
- Gomez J. Detection and diagnosis of the early caries lesion. BMC Oral Health. 2015;15 Suppl 1(Suppl 1):S3. doi: 10.1186/1472-6831-15-S1-S3. Epub 2015 Sep 15. PMID: 26392124; PMCID: PMC4580848.
- Lee Y. Diagnosis and Prevention Strategies for Dental Caries. J Lifestyle Med. 2013 Sep;3(2):107-9. Epub 2013 Sep 30. PMID: 26064846; PMCID: PMC4390741.
- Nokhbatolfoghahaie H, Alikhasi M, Chiniforush N, Khoei F, Safavi N, Yaghoub Zadeh B. Evaluation of Accuracy of DIAGNOdent in Diagnosis of Primary and Secondary Caries in Comparison to Conventional Methods. J Lasers Med Sci. 2013 Fall;4(4):159-67. PMID: 25606325; PMCID: PMC4282000.
- Rashid MF, Karobari MI, Halim MS, Noorani TY. Effectiveness of Visual-Tactile Examination and DIAGNOdent Pen in Detecting Early Enamel Caries and Its Remineralisation: An In Vitro Study. Biomed Res Int. 2022 Jan 11;2022:1263750. doi: 10.1155/2022/1263750. PMID: 35059458; PMCID: PMC8766177.
- Kühnisch J, Heinrich-Weltzien R. Quantitative light-induced fluorescence (QLF)–a literature review. Int J Comput Dent. 2004 Oct;7(4):325-38. English, German. PMID: 16124501.
- Sharma R, Ghambir N, Gupta N, Singh R. Comparative Evaluation of Different Varnishes and Pit and Fissure Sealants on Streptococcus mutans Count in Saliva of Children. Int J Clin Pediatr Dent. 2022 May-Jun;15(3):362-365. doi: 10.5005/jp-journals-10005-2385. PMID: 35991797; PMCID: PMC9357540.
- Patel M. Dental caries vaccine: are we there yet? Lett Appl Microbiol. 2020 Jan;70(1):2-12. doi: 10.1111/lam.13218. Epub 2019 Oct 9. PMID: 31518435.
- Shivakumar K M, Vidya S K, Chandu G N. Dental caries vaccine. Indian J Dent Res [serial online] 2009 [cited 2022 Nov 13];20:99-106. Available from: https://www.ijdr.in/text.asp?2009/20/1/99/49066














Comments