Abstract
Taurodontism can be defined as a change in tooth shape caused by the failure of Hertwig’s epithelial root sheath diaphragm to invaginate at the proper horizontal level.1 Taurodontism appears most commonly as an isolated anomaly, though its association with several syndromes and abnormality has also been reported. A case of a 25 year old female with taurodontism in a tooth is reported here. Endodontic treatment was indicated due to irreversible pulpitis. This article describes the procedure of root canal treatment of mandibular right second molar with taurodontism.


Introduction
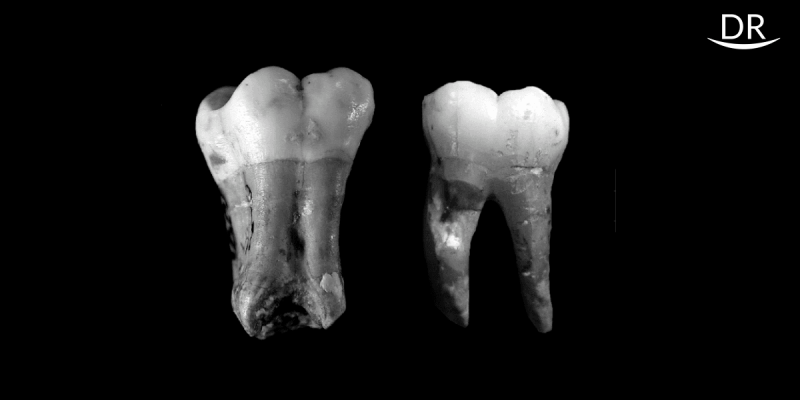
In taurodontism, the body of the tooth is enlarged at the expense of root (also called as ‘bull-like’ tooth). Pulp chamber is extremely large with greater height apico-occlusally. Bifurcation or trifurcation may be present only few millimetres above the root apex and pulp usually lacks constriction at cervical level of tooth.2 Although permanent molars are more commonly affected, this change can be seen in both permanent and deciduous dentition, unilaterally or bilaterally , and in any combination of teeth and quadrant.1

Etiology: Theories regarding the etiology of taurodontism have been many. It’s been suggested that the anomaly represents a primitive pattern , a mutation, a specialized odd retrograde character , an atavistic feature, an X-linked trait, familial or an autosomal dominant trait. 1 Taurodontism can represent itself as a single entity or as a part of a syndrome . This condition is commonly seen in association with certain syndromes like Klinefelter syndrome and Down’s syndrome. 2
Classification : Shaw (1928) classified taurodont teeth according to their severity into –
- hypo- taurodont
- meso- taurodont and
- hyper-taurodont forms.
Hypotaurodontism is the least pronounced form, mesotaurodontism is the moderate form and hypertaurodontism being the most severe form in which the bifurcation or trifurcation occurs near the root apices.3
Review of literature shows a wide range in different population. Usually radiographic examination can reveal taurodontism because of its unique appearance with greater apico-occlusal height of pulp chamber and short roots.
Case Report
A 25 year old female who had non contributory medical history, was referred with the chief complaint of spontaneous, severe pain and food lodgement in right mandibular region. Intraoral clinical examination revealed normal shaped crown with deep carious lesion in mandibular right second molar. Tooth was tender on percussion . On performing the vitality test , complete pulpal necrosis was confirmed.
Radiographic examination revealed an abnormal tooth anatomy.
The radiographic findings were:
- Large occlusal carious lesion reaching distal pulp horn.
- The large pulp chamber with pulp stone was extended beyond cemento-enamel junction with greater apico-occlusal height.
- Two short roots were seen.
From radiographic findings , the tooth was diagnosed to be taurodont. Taurodontism on the contralateral side was confirmed by radiograph. All clinical and radiographic findings were suggestive of irreversible pulpitis.

Endodontic Management of Mandibular Right Second Molar:
The tooth was anaesthetised with 2% lidocaine, the access was opened and modified. The pulp stone was removed with the help of an ultrasonic scaler tip and spoon excavator, and remaining pulp tissue was extirpated. The pulp was large and voluminous so to ensure complete removal , 3% sodium hypochlorite was initially used as an irrigant to soften and dissolve the necrotic pulp .
Once the pulp was extirpated , further irrigation was done with normal saline. The pulp chamber was huge and the floor of the chamber could barely be visualised so initially two canal orifices were found at furcation area: distal and mesial. With little efforts all initial 3 files were set into the canal and working length determined with electronic apex locator (EAL) and confirmation radiograph was taken. Here, radiograph played an important role as it showed both the mesial files were in mesiobuccal (MB) canal and there was a radiolucent line along the mesial files in radiograph, suggestive of a mesiolingual (ML) canal. Long rectangular shape of pulp chamber seemed to cause poor visibility and difficulty in locating mesiolingual ML canal as it was Vertucci type V 1-2 type of canal configuration.

To locate the ML canal , first the MB canal was prepared first upto 20 no. with -4% Flexicon rotary files. Then, MB canal was blocked with no. 20k file , and no. 10k file was precurved at the tip, curvature was marked on stopper and inserted slowly into the ML canal in watch-winding motion. Working length for ML canal was measured with EAL and confirmed with radiograph.

Instrumentation was carried out using Neoendo glide path and a Flexicon rotary endodontic file system. The distal canal was instrumented upto 35 no.-4% taper and both the mesial canals were instrumented upto 30 no. -4% taper. Canals were irrigated well with3% sodium hypochlorite during and after biomechanical preparation to ensure complete removal of necrotic pulp. Calcium hydroxide powder with normal saline was used as an intracanal medicament and access cavity was sealed with temporary filling material.
Few days later, at the time of second appointment, patient was asymptomatic. Root canals were irrigated well with 3% sodium hypochlorite, normal saline and 17% EDTA . After drying the canal , obturation was performed using cold lateral condensation technique with Sealapex sealer and access cavity was sealed with final restoration. The final radiograph confirmed well obturated canals.

Discussion
Clinically, taurodontism can't be differentiated from normal tooth as its body and root lies below alveolar margin. The only means of diagnosis is a radiographic investigation.
The distance between baselines connecting two CEJ and highest point in floor of pulp chamber are used in determining taurodontism. It's diagnosed in molars when this distance exceeds 2.5 mm. 3 According to the classification mentioned previously, presented case can be classified as ‘mesotaurodont’. Taurodontism presents a great challenge in endodontic treatment while negotiating the canal orifice, instrumentation and while obturation probably due to –
- size and shape of pulp chamber
- poor visibility
- proximity of root canals
- apical displacement of root
- voluminous pulp and
- varying degree of obliterations.
In the case presented, additional problems encountered were –
- BMP was time consuming due to typical internal anatomy
- both the mesial canals were narrow
- orifices were too close to each other and
- orifices were placed deeply in tooth.
Conclusion
The present case describes successful completion of endodontic treatment of mandibular right second molar with taurodontism. Radiographic examination is very important because in taurodontism access cavity is usually deeper than normal tooth and pulp is also voluminous and large, so if we don't have a proper radiograph it may be confused with perforation. Careful evaluation for detecting all the canals is also crucial. Endodontic treatment of taurodontism is often challenging and needs more time than normal tooth.
References
- Manjunatha BS, Kovvuru SK. Taurodontism –A Review on its etiology, prevalence and clinical considerations. JClin Exp Dent. 2010;2(4):187-90.
- Garg N, Garg A. Textbook of Endodontics. 3rd ed. Jaypee,(year)
- Bhartiandra A, Tikku A P, Wadhwani KK. “Taurodontism” an endodontic challenge: a case report. INT J ORAL SCI. 2009;51(3):471–4.















Comments