
(This article is co-authored as a collective study by Dr Mriganka Sekhar Ghose, Dr Adhikansh jaggi, Dr Ruqaiyah johar, Dr M.D. Manzur Ahmed, Dr Brijesh singh, Dr Kowshik. V, Dr Naga S. L., Dr Pranavi Nittala, Dr Arra Goutham Kumar, Dr Priya Jha, Dr Harinikhita, Dr Rashid Ali, Dr Shubham Jain, Dr Sourav Dutta, Dr Asif Ali Mudgal, Dr Rupali R Patwekar)


Abstract
Bell’s palsy is a condition that causes temporary facial paralysis (palsy). It usually only affects the muscles on one side of the face. Facial nerve palsy scarcely occurs as a rare complication of inferior alveolar nerve block (IANB) injection which is often carried out in dental procedures being performed in the lower jaw11. This article’s purpose is to report how commonly facial paralysis is encountered by dental professionals after inferior alveolar nerve blocks. A survey involving 233 dentists from different parts of India was conducted to determine the number of dentists who come across this complication in their practice.

Introduction
The term facial palsy generally refers to weakness of the facial muscles, mainly resulting from temporary or permanent damage to the facial nerve 1,2. The facial nerve is important for expression of emotion and communication, and ay significant damage to this nerve can lead to a worsening quality of life 3. Facial paralysis occurs when the facial nerve (cranial nerve VII) gets injured, and subsequently results in asthenia, drooping and loss of facial movement on one side (unilateral) or both sides (bilateral) of the face. Possible causes for facial palsy include inflammation, trauma, stroke, or tumours. 4 It may also occur without a known cause, which is referred to as Bell’s palsy.
During extraction of the mandibular posterior tooth, inferior alveolar nerve block (IANB) is usually administered. One of the important complications of IANB is facial palsy.5 Facial nerve paralysis might be portrayed in 2 ways depending on the onset of palsy; immediate and delayed.6
- Immediate facial nerve palsy occurs due to direct injection of anaesthetic solution touching the facial nerve usually followed by an intra-glandular injection into the parotid gland. It is observed within minutes following the injection and subsides within a few hours.
- On the contrary, the delayed type could be a result of an ischemic paralysis in the stylomastoid foramen region led by a sympathetic vascular reflex. It is important to consider the possibility that it could be attributed to central nervous system involvement in the delayed type.
A rare possibility of facial nerve paralysis could be due to stretching of the facial nerve during lengthy dental procedures where the mouth is kept open for a long time. Symptoms usually appear from several hours to several days after an administration of local anaesthesia and recovery for a delayed response can take 24 hours to several months. Occasionally there is delayed onset and prolonged recovery. Furthermore, varied anatomy can be attributed to posing a higher risk of facial palsy due to IANB.1
Material and Method
An online questionnaire and face-to-face interview-based survey was conducted to identify the prevalence of facial palsy as a complication of inferior alveolar nerve block.
Data collection procedure and tools
Before the start of the survey, education and training of the fifteen examiners was conducted to ensure uniformity and eliminate examiner bias.
Survey interview
Assessment was done using a questionnaire consisting of some closed and open-ended questions like the gender of the dental practitioner, his/her demographic details, and his/her qualification; and one close-ended question – “Did any of your patients ever come back to you complaining that he she suffered facial paralysis a few hours after you gave the inferior alveolar nerve block for extraction of his/her tooth?”
Result
A survey including 233 dentists from different parts of India was conducted to determine the number of dentists who had observed facial palsy after an inferior alveolar nerve block. Of the participants, 116 were male and 117 were female dentists. Among them, 130 were BDS dentists, 87 were MDS dentists, and 16 were interns/students.
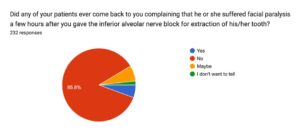
Among all the dentists 85.8% (199) had never seen any complication of facial palsy, 5.6%(13) had seen the complication, and 8.6% (20) were either not willing to tell or were unaware of the symptoms.
Discussion
A total of 233 dentists were included in the survey, and confirmation of facial palsy after IANB was considered based on the judgment of the practitioner filling out the survey form. The fifteen trained examiners guided the dentists through a face-to-face interview ensure uniformity and eliminate examiner bias.
This survey was aimed to find out how many people suffer from facial palsy as an after-effect of the regular nerve block technique used for the extraction of mandibular molar (IANB), as facial palsy is a known complication of this nerve block. Facial palsy can occur due to multiple reasons 4, but this research survey aims on the facial palsy after IANB anaesthesia, which can be seen as it’s complication. Finding out the frequency of occurrence of the facial palsy after IANB will help in determining a better treatment plan for the complication, anticipation of the risk before giving the block, management of the complication and counselling of the patient for consent.
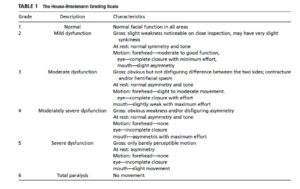
The result of the survey shows that 13 dentists out of 233 have seen the complication of IANB as facial palsy, which is a very rare condition. No significant co-relation was found between the dentist’s demography, gender, qualification and observation of the complication. Clinically, facial palsy presents the following clinical features (Table 1)7
Clinical evaluation
Evaluation of the case is based on the following steps 8
- History taking for the site, onset, characteristics, and duration of the condition with the amount of recovery is important.
- Facial examination at rest and in motion for analysing mimetic muscle tone and symmetry, while differentiating between weakness(paresis/hemiparesis) and total flaccidity(paralysis). This includes:
- Forehead- symmetry of wrinkling – the patient is asked to raise an eyebrow
- Orbicularis oculi- helps in complete closure of eyelid – patient with negative upward rotation and exposure of sclera
- Perioral muscle – forced a smile – inability to blow – asymmetry in a smile – the patient is asked to smile
- Nasolabial fold – Depth of nasolabial fold
- Platysma muscle – symmetric contraction of the muscle
- Lingual nerve – the sensation of taste – using sweet, salty, bitter and acidic foodstuff to elicit the tastes on the anterior ⅔ of the tongue.
- CT scan – for fracture
- MRI scan – for any intracranial lesion
- Nerve excitability test – Acute injury
Management
Management of the case is based on the following protocols 8
- Temporary –
Usually done for eye 1 –
- Artificial tears
- eye ointment
- moisture chamber
- taped eyelid
- external eyelid weight
- Botulinum toxin
- temporary tarsorrhaphy
- punctal occlusion.
- Permanent –
- Upper eyelid – Gold weight insertion 9, pretarsal fixation 10, Arion sling 11, temporalis muscle transfer 12.
- Lower eyelid – Lower eyelid and canthal resuspension 8, lateral tarsal strip13, Medial canthal tendon plication 8, sub orbicularis oculi fat (SOOF) lift 14, autogenous facial sling 15,
- Facial Synkinesis – botulinum toxin 8
- Neuromuscular facial retraining 15
- Free nerve muscle graft 8
- Ipsilateral Nerve transposition 8
Limitation
The limitation of this research is that only 233 dentists participated into the survey. To come to a strong conclusion, that facial palsy after IANB anaesthesia as a very rare complication, we need to increase the sample size.
Conclusion
Facial nerve palsy, a known complication of IANB anaesthesia, is a rarely reported complication. It can be either immediate or delayed. The purpose of this article is to identify the number of cases of either immediate or delayed facial palsy as a result of IANB anaesthesia administration. Here considering 233 dentists only 5.6%(13) have seen the complication, and 8.6% (20) were doubtful, while the occurrence of the complication is rare, clinicians should remain cautious that such dental procedures, like giving IANB anaesthesia, can result in facial nerve palsy.
All precautions should be maintained during the administration of the anaesthetic solution.
The conclusion of the survey requires participation from practitioners all over the world to anticipate the frequency more clearly, following this result it can be concluded that palsy can occur due to the IANB nerve block which has various reasons like wrong technique or unique anatomy, which requires clinicians attention and technique sensitivity.
The survey findings prove that complications can be seen with the inferior alveolar nerve block, and require better treatment and observations for the IANB anaesthesia.
References
- BTzermpos FH, Cocos A, Kleftogiannis M, Zarakas M, Iatrou I. Transient delayed facial nerve palsy after inferior alveolar nerve block anaesthesia. Anesth Prog. 2012 Spring;59(1):22-7. doi: 10.2344/11-03.1. PMID: 22428971; PMCID: PMC3309298.
- Facial Palsy UK. (2022, February 14). What is Facial Palsy? – Facial Palsy UK. https://www.facialpalsy.org.uk/inform/what-is-facial-palsy/
- Coulson SE, O’dwyer NJ, Adams RD, Croxson GR. Expression of emotion and quality of life after facial nerve paralysis. Otol Neurotol. 2004 Nov;25(6):1014-9.
- Walker NR, Mistry RK, Mazzoni T. Facial Nerve Palsy. [Updated 2023 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549815/
- Malamed, S. F. (2019, June 3). Handbook of Local Anesthesia. Mosby.
- Chisci G. Facial Nerve Palsy after Inferior Alveolar Nerve Block: A Rare Presentation of Ocular Complication and Literature Review. Reports. 2023; 6(4):47.
- House JW, Brackmann, DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985; 93:146–147.
- Mavrikakis I. Facial nerve palsy: anatomy, aetiology, evaluation, and management. Orbit. 2008;27(6):466-74.
- Saleh GM, Mavrikakis I, et al. Corneal astigmatism with upper eyelid gold weight implantation using the combined high pretarsal and levator fixation technique. Ophthal Plast Reconstr Surg. 2007; 23:381–383.
- Caesar RH, Friebel J, et al. Upper lid loading with gold weights in paralytic lagophthalmos: A modified technique to maximize the long-term functional and cosmetic success. Orbit. 2004;23:27–32.
- Arion HG. Dynamic closure of the lids in paralysis of the orbicularis muscle.Int Surg. 1972; 57:48–50.
- Masters FW, Robinson, DW, et al. Temporalis transfer for lagophthalmos due to seventh nerve palsy. Am J Surg. 1965; 110:607–611.
- Anderson RL, Gordy DD. The tarsal strip procedure. Arch Ophthalmol.1997; 97:2192–2196.
- Horlock N, Sanders R, et al. The SOOF lift: Its role in correcting midfacial and lower facial asymmetry in patients with partial facial palsy. Plast Reconstr Surg. 2002; 109:839–849; discussion 850-854.
- Lee V, Currie Z, et al. Ophthalmic management of facial nerve palsy. Eye.2004; 18:1225–1234.















Comments