– Dr Kalpna Chaudhry


Keywords: MIS-C, Paediatric dentist, covid 19

Introduction
The whole world is struggling with COVID 19. Now in India, the 2nd wave is even more dangerous than the first one and predictions says that 3rd wave will come in the month of September – October and this time children will be more affected for which government is taking some important decisions to face the conditions .
COVID 19 seems to usually cause milder infection in kids than in adults and older people. But some children have developed more serious symptoms, sometimes several weeks after being infected with the virus. This is known as multisystem inflammatory syndrome in children (MIS-C), also known as pediatric inflammatory multisystem syndrome.
What is MIS-C?
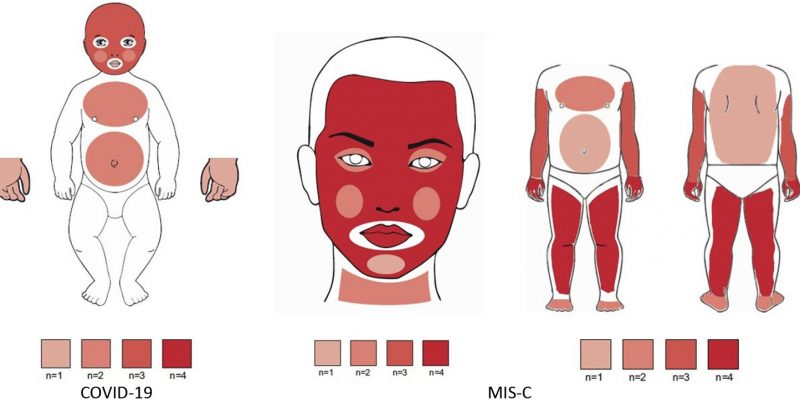
Typically, school aged children are affected (median age 8 years), though MIS-C has been reported in children from infancy through young adulthood. Children with MIS-C present with oral manifestations like reddened lips and swollen tongue, may visit pediatric dentist also for the concern. Patients with MIS-C may present with some features consistent with Kawasaki disease (particularly fever and mucocutaneous changes); however, MIS-C is likely a distinct clinical entity. Patients with MIS-C often have predominant cardiac dysfunction and gastrointestinal symptoms, in addition to biomarker and cytokine differences that appear distinct from Kawasaki disease. One study observed that younger patients (aged 0-5 years) with MIS-C were more likely to meet the disease criteria of typical or atypical Kawasaki disease compared with adolescents (48% v 12%), had a higher prevalence of mucocutaneous symptoms (87% v 62%), and had a lower prevalence of myocarditis (39% v 73%) or neurological symptoms (13% v 39% of adolescents).
Though there are hypotheses around risk factors for MIS-C, such as lower pre-existing immunity to coronaviruses, specific risk factors for developing MIS-C in children are not well established.
The link between COVID-19 and MIS-C is not well understood, and we are trying to learn if some children are more at risk. However, the American Academy of Pediatrics (AAP) wants to reassure parents that very few children get severely ill from the virus that causes COVID-19. So far, most children who have been diagnosed with MIS-C have recovered after getting medical care.
Clinical Symptoms Of MIS-C :
A study published in the March 2021 issue of the Journal of the American Dental Association, reports oral or oropharyngeal symptoms in about half of the 47 MIS-C cases.
They found
- Systemic rash in 32 cases (68.1 %)
- Conjunctivitis in 27 cases (57.5%)
- Cranial nerve palsy in 6 cases (12.8%)
- Red, cracked lips in 23 cases(48.9%)
- Strawberry tongue in 5 cases (10.6%).

Diagnosis
MIS-C symptoms can be similar to those caused by other illnesses, such as Kawasaki disease or toxic shock syndrome. If a doctor thinks a child might have MIS-C, they will do tests that look for signs of inflammation in the body. These can include:

- Blood tests and urine tests
- COVID-19 test
- Chest X-ray/HRCT
- Tests to look at the heart, such as ECG (electrocardiogram) and echocardiogram (ultrasound of the heart)
- Abdominal ultrasound (ultrasound of the belly)
Therapeutic And Preventive Measures
Therapeutic Measures:
Children with mild acute COVID-19 benefit from usual supportive care measures, including rest, hydration, and antipyretics as needed.
Dexamethasone was shown to decrease mortality in adults with moderate to severe respiratory distress, and may be considered in children with significant respiratory illness, though pediatric data are still forthcoming.
Similarly, though efficacy is still being evaluated in children, remdesivir may be prescribed for children with respiratory deterioration.
Other treatments, such as convalescent plasma or monoclonal antibodies, might be considered in high risk patients, but these therapeutics require further study in adults and children.
Children with MIS-C most commonly are treated with intravenous immunoglobulin and often steroids. Data on outcomes and treatment efficacy is limited overall. However, a recent retrospective cohort study (2020) in France found that children with MIS-C who were treated with both intravenous immunoglobulin (IVIg) and methylprednisolone had a lower risk of treatment failure compared with those treated with IVIg alone. Further study is still needed to understand the pathophysiology of MIS-C to inform the most effective therapeutic interventions.
Preventive Measures:
Primary measures to prevent infection and transmission of SARS-CoV-2 remain important for children and their families, and include basic steps such as
- face masks for children aged 2 years and older,
- social distancing, and
- hand hygiene for both children and the adults around them.
Young children or those with developmental delays may not tolerate or wear masks properly; however, there is value in practising. Several vaccines have been authorised for emergency use in persons ≥16 or 18 years. Given that the risks associated with SARS-CoV-2 are much lower in children than in adults, initial studies and vaccine distribution did not prioritise children. Fortunately, several studies are now enrolling younger children as it will be important to understand vaccine safety and efficacy before vaccines are widely administered to younger age groups. Patients should maintain routine preventive care and vaccination schedules, including seasonal influenza vaccine, as a critical strategy to stay healthy during and beyond the pandemic.
Families should continue to follow infection prevention measures, even after individual vaccination, until community rates are low to avoid the potential for asymptomatic transmission to others.
Conclusion
The incidence of MIS-C is likely to increase as the COVID-19 pandemic continues to evolve. Oral changes among patients with diagnosed MIS-C were seen with relative frequency. Dentistry can play an integral role in the early detection of oral manifestations of MIS-C, and dentist should be willing to evaluate high-risk patients.














Comments