

Ankyloglossia, also known as tongue-tie, is a congenital anomaly characterized by an abnormally short lingual frenulum. Its prevalence is around 4.4% to 4.8% in newborns, with a male to female ratio of 3:1. In children, ankyloglossia can lead to breastfeeding difficulties, speech disorders, poor oral hygiene and bullying during childhood and adolescence.

Treatment includes 2 surgical procedures:
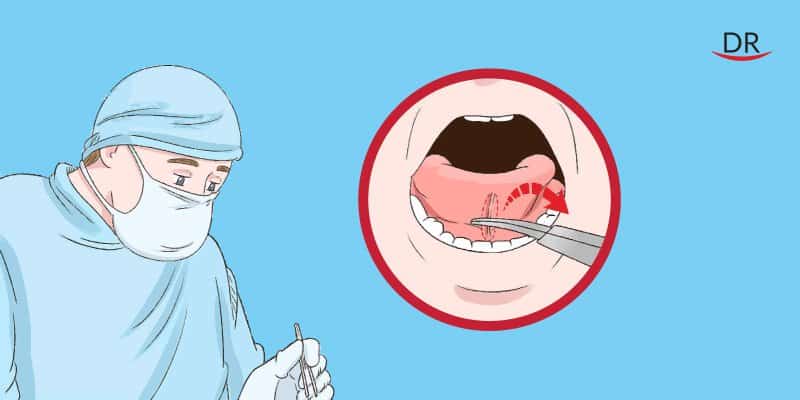
Frenotomy (the clipping of the lingual frenulum) is the most indicated technique for babies with ankyloglossia since it is a conservative, simple and quick procedure that may be performed in the dental office settings during initial consultation. The limitation of this technique is the possibility of recurrence and the need to perform complementary procedures to release the tongue satisfactorily.
Frenectomy corresponds to the complete excision of the frenulum. This procedure is more invasive and difficult to be performed in young children, although the results are more predictable, decreasing the recurrence rate. Surgery should be performed before the child develops abnormal swallowing and speech patterns and if performed in older children, they should be referred to a speech therapist in order to reestablish the normal functions of the tongue
Demographic data
A 6 year old male patient, born in Moradabad, UP, India, reported to the clinic in 2016 with a chief complaint of difficulty in speech.
The patient was completely asymptomatic when his parents realized that he had an interrupted speech and he could not pronounce certain words. Patient’s mother first identified the problem. They have visited several dentists and physicians and they were told their was child was perfectly normal and the problem will resolve with age.
Prenatal History
No relevant history of the mother regarding illness or trauma during pregnancy was reported. No drug therapy was taken before he was born.
Natal History
- The delivery was full term and caesarian type of delivery was performed.
- There was no history of jaundice or cyanosis at birth.
- There was no history of blood transfusion.
Post natal history
- The milestones of development were normal.
- Patient was immunised with triple vaccine.
- There was no history of injuries, minor/major accidents or food/drug allergy.
- Patient has a sibling, one elder sister who did not suffer from this problem.
Personal history– History of consanguinous marriage was not reported. His sibling or near relative was also not suffering from this anomaly.
PAST MEDICAL HISTORY: No relevant history reported.
PAST DENTAL HISTORY: Third visit to a dental clinic; first visit to our dental hospital.
Diet history ( 3 days):
- Morning – milk and biscuits ( one spoon sugar )
- Lunch – rice, dal, vegetables
- Evening- milk and biscuits ( one spoon sugar )
- Dinner – same as lunch
- Intake of sugar is more.
- Patient is fond of toffees, chocolates and sugary fruit juices.
General Physical Examination:
- GAIT: No Abnormality Reported
- BODY TYPE: Mesomorphic
- POSTURE: Erect
- BUILT: Aesthetic
- HEIGHT: 3 feet
- WEIGHT: 20 Kg
- SHAPE OF HEAD: Mesocephalic
- FACIAL FORM: Oval
- FACIAL SYMMETRY: bilaterally symmetrical
- FACIAL DIVERGENCE: Straight
Extra Oral examination:
- No Abnormality Detected In skin, hair line, Eyes, Ears, Nails, Hair, Lymph Nodes.
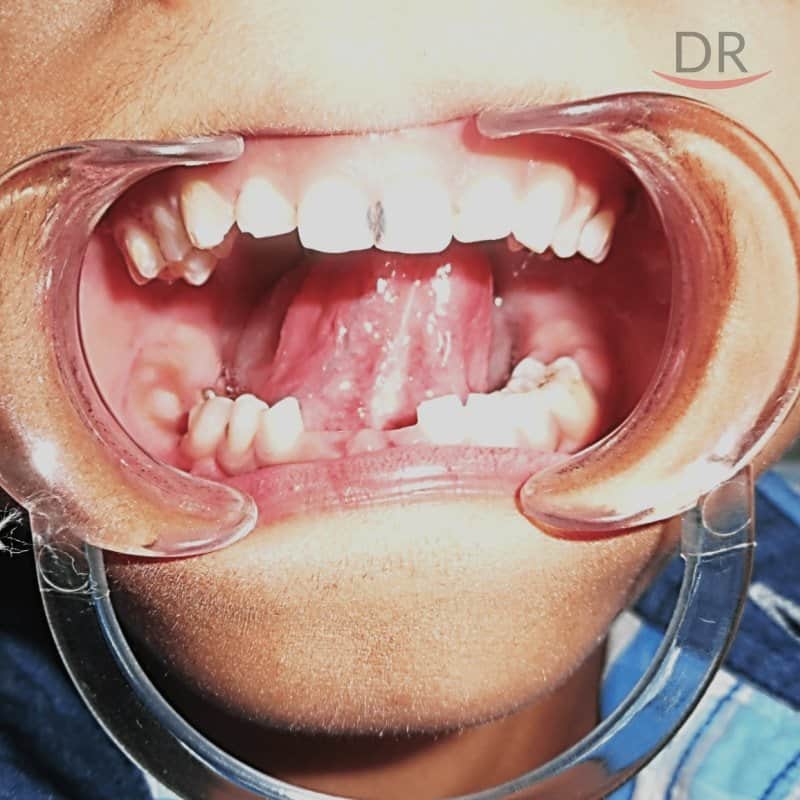
Intra oral examination
- No abnormality was detected on rest of the Mucosa, Palate, Floor of the Mouth, Salivary Gland, Lymph Nodes and Buccal Mucosa.
- GINGIVA– Pale pinkish in color scalloped with round margins.
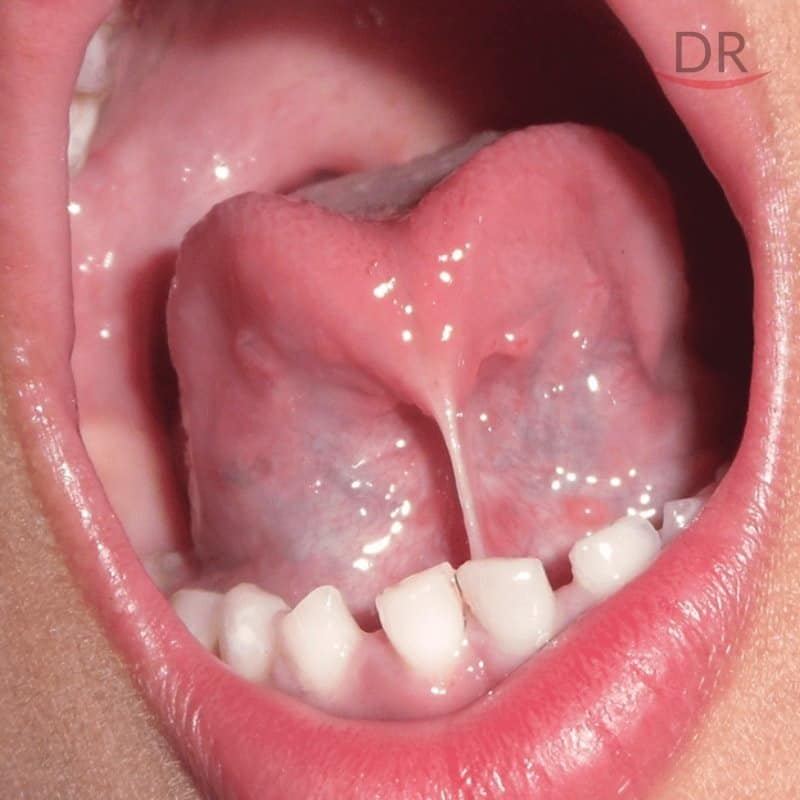
- High lingual frenal attachment


Hard Tissue examination
Teeth present
55 54 53 52 51 61 62 63 64 65
75 74 73 72 71 81 82 83 84 85
Stains/calculus- +/+
Carious: 51 61
Pre-exfoliative mobility irt 71, 81
Diagnosis: Tongue tie
Treatment plan:
- Emergency phase of treatment was not required. Medical/Systemic phase was also not required.
- For the preventive phase of treatment, oral hygiene instructions were given.
- For the preparatory phase, oral prophylaxis was performed.
- For the corrective phase, lingual frenectomy was performed using diode laser (pictures given below). Restoration of 51, 61 was planned and performed.
- The maintenance phase consisted of periodic recall and compulsory follow up after one day and one week (pictures given below).
Corrective Phase:

Intra oral and extra scrubbing
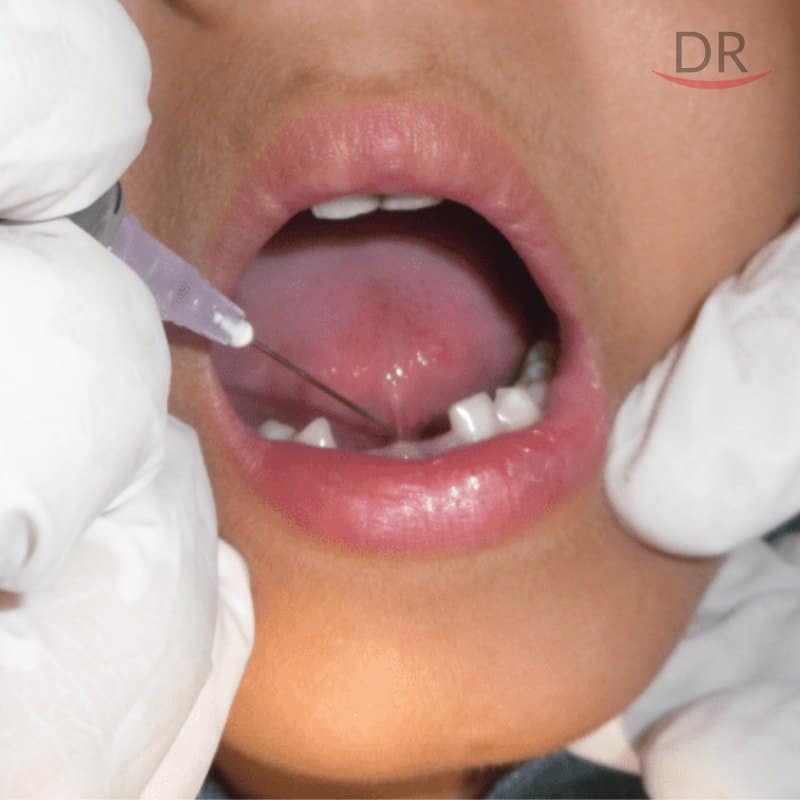
Aministration of local anesthesia

Suture placed to stabilize the tongue

Diode laser frenectomy done

After frenectomy

Immediate post-op

Instructions and oral physiotherapy :
The patient was discharged with analgesics (as and when required).
The following exercises were advised:
- Stretch the tongue up towards the nose, then down towards the chin and repeat,
- Open the mouth widely and touch the big front teeth with the tongue with mouth still open,
- Close the mouth and poke the tongue into the left and right cheek to make a lump for 3 to 5 minute, 3 – 4 times a day for 3 or 4 weeks post-operatively.
Maintenance phase:

Next day
After 1 week
pre-op

Post-op
Discussion:
- Ankyloglossia or “tongue‑tie” is a congenital anomaly caused by an abnormally thick , tight lingual frenulum (the band of tissue that connects the tongue base to the floor of the mouth) resulting in limitation of tongue movement.
- Wallace defined Ankyloglossia (tongue tie) as “a condition in which the tip of the tongue cannot be protruded beyond lower incisor teeth because of a short lingual frenulum, often containing scar tissue”.
- Ankyloglossia leads to inability to extend the tip of tongue beyond the vermillion border of the lips or a line joining the lip commissures, along with speech impairment, oral motor dysfunction and mandibular lingual gingival recession.
Diode Laser:
- Diode lasers are excellent coagulators. Because the energy is not confined in the spatial parameters of the blood vessels, the clinician must work fast.
- Application technique is critical.
- Accurately providing de-epithelialization is virtually impossible. Epithelium is only 100 to 300 microns in thickness. Only 5% of diode energy gets absorbed by the epithelium, and 95% is absorbed into the submucosa with penetration depth up to 10 mm.
- Energy extending greater than 200 to 500 microns can cause thermal damage.
- Necrosis can occur with longer healing times.
References:
- Khairnar M, Pawar B, Khairnar D. A Novel Surgical Pre-suturing Technique for the Management of Ankyloglossia. Journal of Surgical Technique and Case Report. 2014; 6(2)
- Ballard, J.L., Auer, C.E., Khoury, J.C. Ankyloglossia: Assessment, Incidence, and Effect of Frenuloplasty on the Breastfeeding Dyad. Pediatrics 2002;110;e63
- Antony VV , Khan R. "Management Of Ankyloglossia" – Case Reports. J Dent Medical Sci. 2013;6(4) p 31-33.















Comments