
Full mouth rehabilitations (FMR) are comprehensive dental procedures aimed at restoring optimal oral health and function in patients with extensive dental issues. It is considered when a patient presents with a complex set of dental problems that cannot be effectively addressed through isolated treatments. Common scenarios include severe tooth wear, advanced periodontal disease, widespread decay, and multiple missing teeth, affecting their phonetics, esthetics and functional occlusion. Additionally, individuals with temporomandibular joint (TMJ) disorders or occlusal problems may benefit from full mouth rehabilitation to restore harmony in their bite and alleviate associated symptoms. But there is another type of rehab, which addresses only selective issues of functional occlusion and is certainly not as inclusive as a traditional FMR, referred to as a ‘selective rehab’.


Selective rehabs are sometimes frowned upon and are considered controversial in nature, because:

1) It’s a compromised treatment plan, which does not address all dental issues simultaneously.
2) It may or may not prevent the progression of existing problems and the development of new ones.
3) It may or may not contribute to the long-term stability of the patient’s oral health.
That said, there is a small segment of patients who do not fit in the scope of a typical full mouth rehab. These patients show selective wear of teeth, usually on one side only, i.e. only two quadrants rather than four. The reasons for this usually are-
- previous prosthesis fabricated in a wrong plane of occlusion or
- unilateral mastication by the patient eventually leading to damage of the existing prosthesis.
In such patients, the necessity of doing a full mouth rehab does not arise and au contraire would be very aggressive. Treating the quadrants in question, would be more conservative, but also far more difficult, for the practitioner is bound by certain pre-existing constraints and has to find a way to work within them (e.g. existing vertical dimension of occlusion and MIP), and that can be quite tricky.
The decision to pursue a selective full mouth rehabilitation is often made after a thorough assessment by a dental professional. This evaluation includes a comprehensive examination of the patient’s oral health, diagnostic imaging, and discussions about their oral health history, functional concerns, and esthetic preferences. And last but not the least, the financial constraints of the patient. There are patients who have a limited budget, and so we honour that and perform only a selective rehab for the only other solution would be refusal to treat, but these patients are very few and far between for they are also what I like to call ‘border line’ cases. While their functional occlusion is not ideal, it is not severe enough to require intervention in the form of an FMR, then and there and if carefully handled, the latter can be delayed by a few years. While this may seem like a superficial solution at first, if done right, its possible to slow the process of tooth wear and in some cases, even halt it, for a status quo of some sort has been reached in the oral cavity, which is of course aided by the patient’s willingness to understand and follow post-operative instructions.
How is Selective Full Mouth Rehabilitation Performed?
1) Thorough Assessment: The process begins with a comprehensive assessment of the patient’s oral health. This includes a detailed examination, diagnostic imaging (such as an OPG), and discussions about the patient’s concerns and goals including their monetary constraints.
2) Treatment Planning: Based on the assessment, a customized treatment plan is developed, which is usually limited to only one side or two quadrants. The treatment plan may include a combination of restorative, periodontal, endodontic, and prosthetic procedures.
3) Phased Approach: Selective rehabs themselves can be considered as a form of phased dental treatment, allowing the dentist to prioritize and address immediate concerns first rather than potential future ones.
4) Collaboration between Specialists: Some cases may involve collaboration between different dental specialists, such as prosthodontists, periodontists, oral surgeons, and orthodontists. This interdisciplinary approach ensures that each aspect of treatment is expertly handled.
5) Provisional Restorations: Temporary or provisional restorations are placed during the treatment process to maintain function and esthetics while the final restorations are being fabricated. This step is especially important to evaluate the restored functional occlusion and the patient’s adaptation to it.
6) Final Restorations: Once all necessary procedures are completed, final restorations are placed. This may include crowns, bridges, dental implants, or other prosthetic devices to achieve the desired functional and aesthetic outcomes.
I would like to illustrate the above aspects in the form of a case report.
Case Report
A lady in her early seventies entered my operatory with dislodged crown prostheses on 47 and 48 along with the chief complaint of being unable to masticate. She was referred by another clinician to me, specifically for a selective rehab.
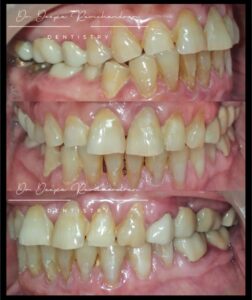

The pre-operative images and OPG show:
- loss of vertical dimension on the right with a complete reverse Curve of Spee.
- loss of soft and hard tissue on the lower incisors.
- grade 1 mobility on 31 and 41; trauma from occlusion.
- attrition on the incisal edge of anteriors (i.e.lack of anterior guidance).
- various cervical abrasion defects.
- uneven zenith and shade mismatch of UL FPD.
After due consideration of all above factors, my final conservative treatment plan was a partial rehab, i.e. I raised the vertical dimension selectively only on the right, to match that on the left.
- The RCT on 46 is not ideal, but as there was no pain and the tooth tested negative for pain on percussion, with no intra oral findings, the patient was not willing to redo.
- In order to correct the plane of occlusion and raise the vertical dimension on the right side, 44 and 45 would need to be prepped to prevent gaps in the corrected occlusal plane.
- To improve retention, a five-unit cad-cam PFM FPD was planned from 44 to 48, with emphasis on maintaining the vitality of the premolars.
- Indirect restorations on 12 and 13 so as to convert the anterior guidance from shallow to steep, but if the patients’ finances did not permit, then lengthening of the incisal edge, chair side, with composite.
- Replacement of UR FPD, as part of phase two of the treatment due to financial constraints. Rehabilitating the lower posteriors first, though not ideal, would help her masticate while she gathered funds for the next phase.
A PMMA temporary FPD on 44-48, fabricated to the corrected plane of occlusion, was utilized to adjust the opposing FPD chair-side.

The LR final prosthesis was then cemented.

Next, 12 and 13 were prepped for full coverage zirconia crowns, to enable me to change the palatal contour. A before and after comparison, shows us the corrections in functional occlusion especially with respect to the plane of occlusion. Note the beautiful gingival adaptation around the LR FPD.

In conclusion, the decision to pursue selective rehabilitation involves a thorough assessment, careful treatment planning, and patient co-operation to ensure effective and manageable care. It is also deceptively more tedious, time consuming and technique sensitive, than it appears, and requires the clinician to have a very through knowledge of functional occlusion, especially as, drastic corrections have to be brought about, but within pre-existing parameters. This necessitates that the clinician understand, that while ideal restoration of occlusion is not possible, every effort must be made to achieve the maximum corrections, within the framework of a selective rehab.











Comments